TREATMENT OF ID IN PATIENTS
WITH HEART FAILURE
Guideline Recommendations
| Iron Deficiency in HF | HFrEF and iron deficiency with or without anemia | 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic HF | ||
|---|---|---|---|---|
|
Target HF population |
HFrEF and iron deficiency with or without anemia |
HF and anemia |
Symptomatic patients with LVEF <45% and iron deficiency, defined as serum ferritin <100ng/ml or serum ferritin 100-299 ng/mlwith TSAT <20% |
Symptomatic HF patients recently hospitalized for HF and with LVEF <50% and iron deficiency defined as serum ferritin <100ng/ml or serum ferritin 100-299ng/mlwith TSAT <20% |
|
Recommendations |
Intravenous iron replacement is reasonable to improve functional status and QOL |
Erythropoietin-stimulating agents should not be used to improve morbidity and mortality |
IV iron supplementation with ferric carboxymaltose should be considered in order to alleviate HF symptoms, improve exercise capacity and QOL |
IV iron supplementation with ferric carboxymaltose should be considered to reduce the risk of hospitalization |
|
IV iron supplementation with ferric carboxymaltose should be considered to reduce the risk of hospitalization |
2a |
3:Harm |
IIa |
IIa |
|
Level of
recommendation |
B-R |
B-R |
A |
B |
Algorithm for screening/diagnosis and treatment/follow‐up of iron deficiency in patients with chronic heart failure.
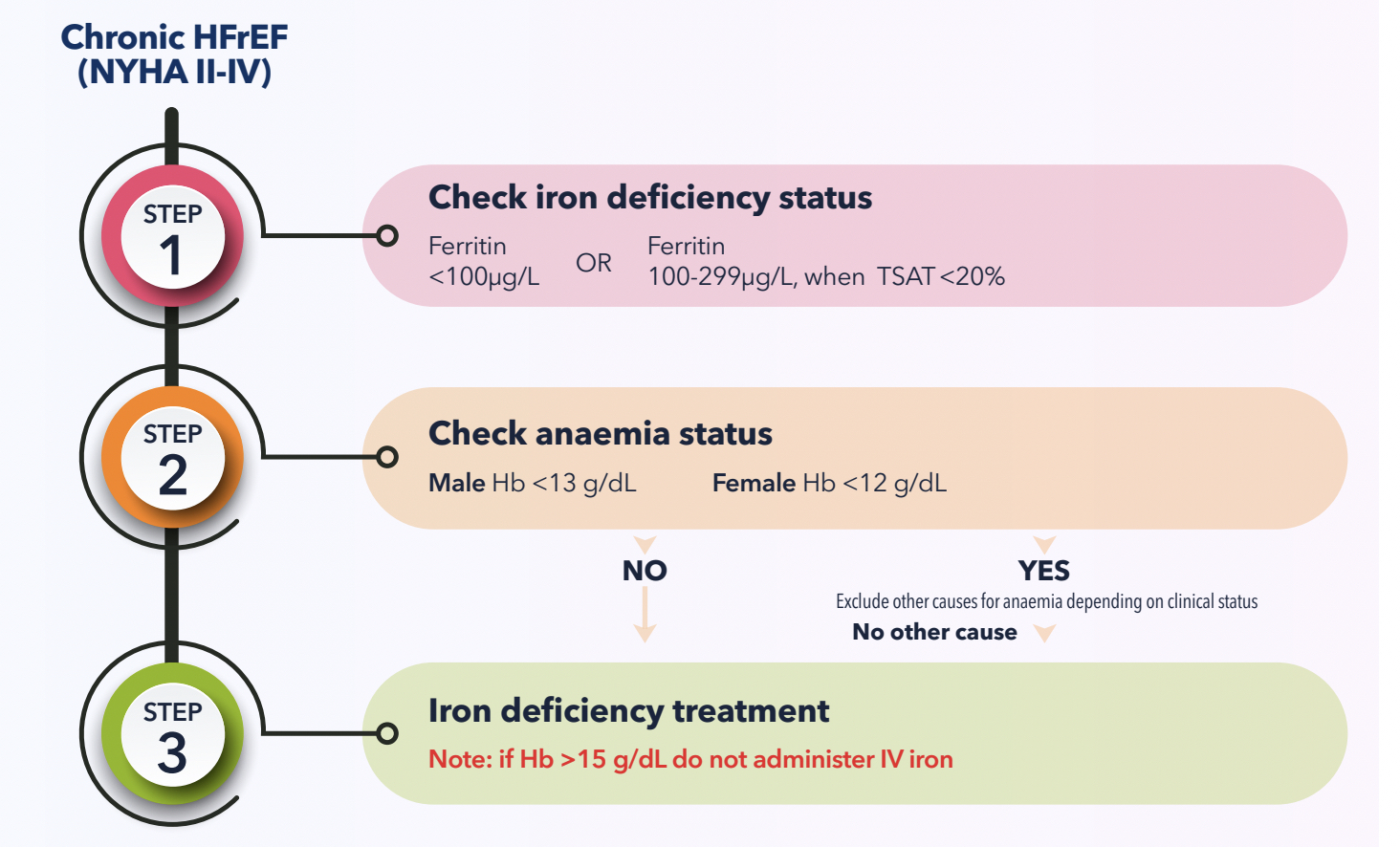
Chronic HFrEF
(NYHA II-IV)
Check iron deficiency status
Check anaemia status
Iron deficiency treatment
Ferritin
<100μg/L
OR
Ferritin
100-299μg/L, when TSAT<20%
Male Hb <13 g/dL
OR
Female Hb <12 g/dL
Note: if Hb >15 g/dL do not administer IV iron
Conisder single doses of ferric carboxymaltose (500-100 mg iron)
to correct iron deficiency*
Calculate total iron need using the table:
| Hemoglobin | Patient body weight | |||
|---|---|---|---|---|
|
g/DL |
mmol/L |
<35 kg |
35 kg to <70 kg |
≥70 kg |
|
<10 |
<6.2 |
500 mg |
1500 mg |
2000 mg |
|
10 to <14 |
6.2 to <8.7 |
500 mg |
1000mg |
1500 mg |
|
≥14 to 15 |
≥8.7 to 9.3 |
500 mg |
500 mg |
500 mg |
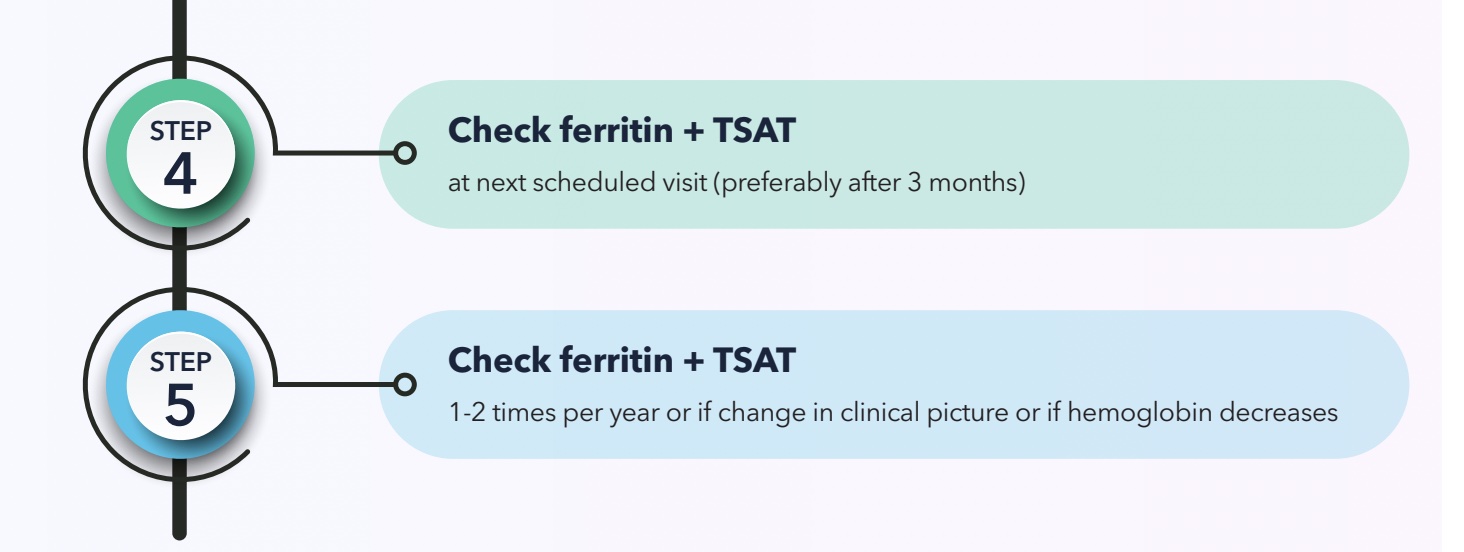

Check ferritin + TSAT
Check ferritin + TSAT
at next scheduled visit (preferably after 3 months)
1-2 times per year or if change in clinical picture or if hemoglobin decreases
Hb = hemoglobin, HF = heart failure, HFrEF = heart failure with reduced ejection fraction, FCM = ferric carboxymaltose, NYHA = New York Heart Association Functional Classification, QOL = quality of life, TSAT = transferrin saturation
Download this article as a PDF
REFERENCES:
- McDonagh, Theresa, et al. “Screening, diagnosis and treatment of iron deficiency in chronic heart failure: putting the 2016 European Society of Cardiology heart failure guidelines into clinical practice.” European Journal of Heart Failure 20.12 (2018): 1664-1672.
- McDonagh, Theresa A., et al. “2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC.” European heart journal 42.36 (2021): 3599-3726.
- Heidenreich, Paul A., et al. “2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines.” Journal of the American College of Cardiology 79.17 (2022): e263-e421.