Poor prognosis independently of anemia and left ventricular ejection fraction
Imparied health-related quality of life (HRQoL)
Iron
deficiency
and exercise
intolerance in
heart failure
Iron deficiency in patients with stable systolic heart failure has been observed to be associated with submaximal exercise capacity as well as endurance.
In hematopoietic tissues, including erythrocytes, immune cells, and platelets
In nonhematopoietic tissues, including myocardium, adipose tissue, liver, kidneys, and brain
In hematopoietic tissues, including erythrocytes, immune cells, and platelets
In nonhematopoietic tissues, including myocardium, adipose tissue, liver, kidneys, and brain
Symptoms related to reduced O²
transportation (i.e. reduced
maximal performance)
Symptoms related to reduced
tissue iron deficiency (i.e.
reduced endurance)
In hematopoietic tissues, including erythrocytes, immune cells, and platelets
In nonhematopoietic tissues, including myocardium, adipose tissue, liver, kidneys, and brain
In hematopoietic tissues, including erythrocytes, immune cells, and platelets
In nonhematopoietic tissues, including myocardium, adipose tissue, liver, kidneys, and brain
Iron
deficiency
and exercise
intolerance in
heart failure
Iron deficiency in patients with stable systolic heart failure has been observed to be associated with submaximal exercise capacity as well as endurance.
In hematopoietic tissues, including erythrocytes, immune cells, and platelets
In nonhematopoietic tissues, including myocardium, adipose tissue, liver, kidneys, and brain
In hematopoietic tissues, including erythrocytes, immune cells, and platelets
In nonhematopoietic tissues, including myocardium, adipose tissue, liver, kidneys, and brain
Anemia
Reduced O²
carrying capacity
(hemoglobin)
Symptoms related to reduced O²
transportation (i.e. reduced
maximal performance)
Symptoms related to reduced
tissue iron deficiency (i.e.
reduced endurance)
In hematopoietic tissues, including erythrocytes, immune cells, and platelets
In nonhematopoietic tissues, including myocardium, adipose tissue, liver, kidneys, and brain
In hematopoietic tissues, including erythrocytes, immune cells, and platelets
In nonhematopoietic tissues, including myocardium, adipose tissue, liver, kidneys, and brain
IRON DEFICIENCY is a key
determinant of health-related
quality of life in heart failure,
regardless of anemia status
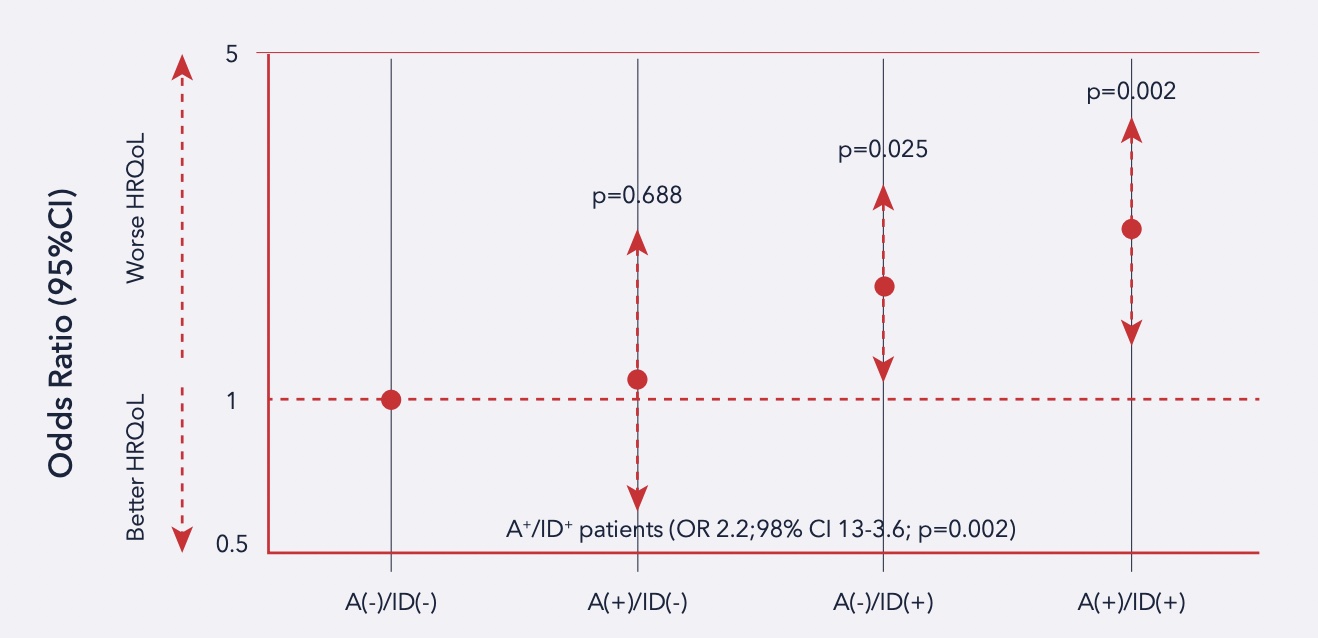
Patients impacted by chronic heart failure (CHF) present significant impairment of health-related quality of life (HRQoL). The role of iron in energy metabolism could be the link between ID and HRQoL.
The worst HRQoL was observed in the presence of anemia as well as iron deficiency. A significant impact on HRQoL was observed in the presence of ID regardless of anemia
The worst HRQoL was observed in the presence of anemia as well as iron deficiency. A significant impact on HRQoL was observed in the presence of ID regardless of anemia
Iron deficiency and
prognosis in heart failure
Studies have found that in patients with systolic HF, ID was a strong independent predictor of death as well as heart transplantation.
Kaplan-Meier
curves
reflecting 3-year
event-free
survival rates in
546 patients
with systolic
heart failure
with vs. without
iron deficiency.
Iron deficiency and
prognosis in heart failure
Studies have found that in patients with systolic HF, ID was a strong independent predictor of death as well as heart transplantation.
Kaplan-Meier curves reflecting 3-year event-free survival rates in 546 patients with systolic heart failure with vs. without iron deficiency.
Kaplan-Meier
curves
reflecting 3-year
event-free
survival rates in
546 patients
with systolic
heart failure
with vs. without
iron deficiency.
REFERENCES: Van Veldhuisen, Dirk J., et al. “Anemia and iron deficiency in heart failure: mechanisms and therapeutic approaches.” Nature Reviews Cardiology 8.9 (2011): 485-493.
Lewis, Gregory D., et al. “Oral iron therapy for heart failure with reduced ejection fraction: design and rationale for oral iron repletion effects on oxygen uptake in heart failure.” Circulation: Heart Failure 9.5 (2016): e000345.
Jankowska, Ewa A., et al. “Iron deficiency: an ominous sign in patients with systolic chronic heart failure.” European heart journal 31.15 (2010): 1872-1880.
Comín‐Colet, Josep, et al. “Iron deficiency is a key determinant of health‐related quality of life in patients with chronic heart failure regardless of anaemia status.” European journal of heart failure 15.10 (2013): 1164-1172.
Anand, Inder S., and Pankaj Gupta. “Anemia and iron deficiency in heart failure: current concepts and emerging therapies.” Circulation 138.1 (2018): 80-98.